
Amy Han, DO | EM PGY3
The Idea:
To develop several grading system prototypes using POCUS and to determine their respective ability to predict acute kidney injury (AKI) after cardiac surgery.
The Study:
This was a prospective cohort study at a tertiary cardiac surgery center from August 2016 to July 2017, of non-critically ill patients 18 years and older undergoing cardiac surgery with the use of cardiopulmonary bypass. All patients underwent POCUS assessment the day before surgery, at ICU admission after surgery, and daily from postoperative days 1 to 3. Each US assessment consisted of hepatic vein Doppler, portal vein Doppler, intra-renal venous Doppler, and inferior vena cava US.
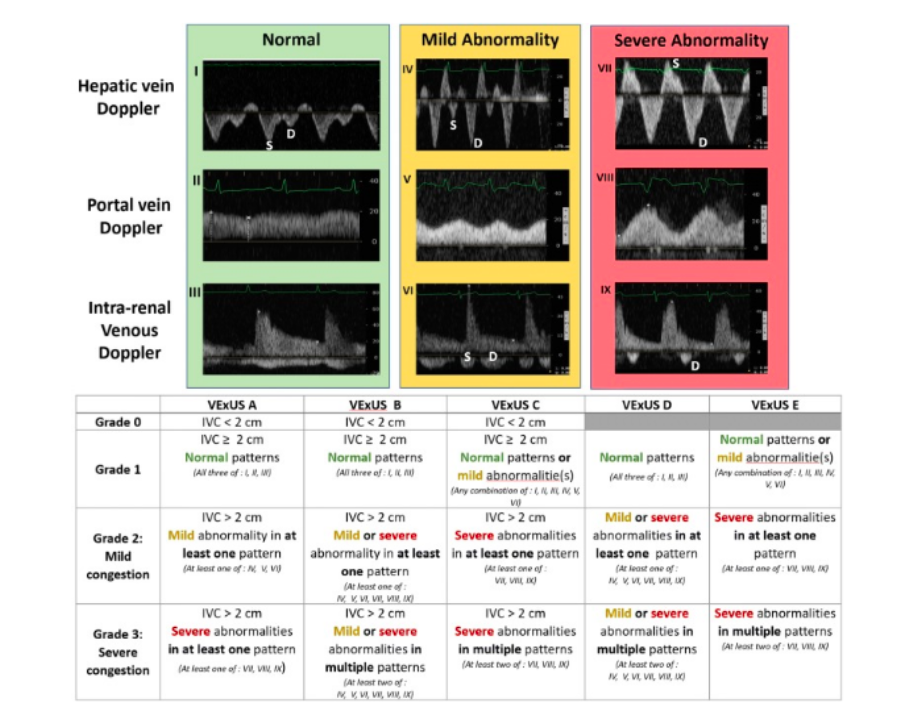
A multidisciplinary team developed five venous excess ultrasound (VExUS) grading system prototypes based on the severity of venous ultrasonographic markers. For hepatic vein Doppler, a systolic phase of lesser amplitude than the diastolic phase but toward the liver was considered mild; the presence of a reversed systolic phase (toward the heart) was considered severe. For portal vein Doppler, a pulsatile fraction (PF, variation in velocities during cardiac cycle) of 30-49% was considered mild; a PF>50% was considered severe. For intra-renal venous Doppler, a discontinuous pattern with a systolic and a diastolic phase was considered mild; a discontinuous pattern with only a diastolic phase was considered severe. The prototype grading systems were named VExUS “A” through “E”. The VExUS score was determined for all patients and for all timepoints.
The Findings:
A total of 705 US assessments from 145 participants were analyzed. The association between each score and AKI was assessed using time-dependent Cox models. In post-operative period, severe congestion (Grade 3) defined by the VExUS C grading system was the most strongly associated with AKI (HR 3.69, CI 1.65-8.24, p=0.001). This association remained significant after adjustment for baseline risk for AKI and vasopressor/inotropic support (HR 2.82, CI 1.21-6.55, p=0.02). At time of ICU admission after surgery, severe congestion (Grade 3) defined by the VExUS C grading system had high specificity (96% CI 89-99%) but low sensitivity (27% CI 15-41%) for development of subsequent AKI, resulting in a moderate positive likelihood ratio of 6.37 (CI 2.19-18.5) which outperformed the use of common central venous pressure cut-offs. In comparison, IVC dilatation alone had poor diagnostic performance (specificity 41%), suggesting that this commonly used US assessment is not sufficient to detect clinically significant congestion.
The Takeaway:
Severe congestion, defined as the presence of severe flow abnormalities in multiple Doppler patterns with a dilated IVC (VExUS grading system C - Grade 3), offered the strongest association with the development of subsequent AKI. POCUS may enable the clinician to detect clinically significant systemic venous hypertension.